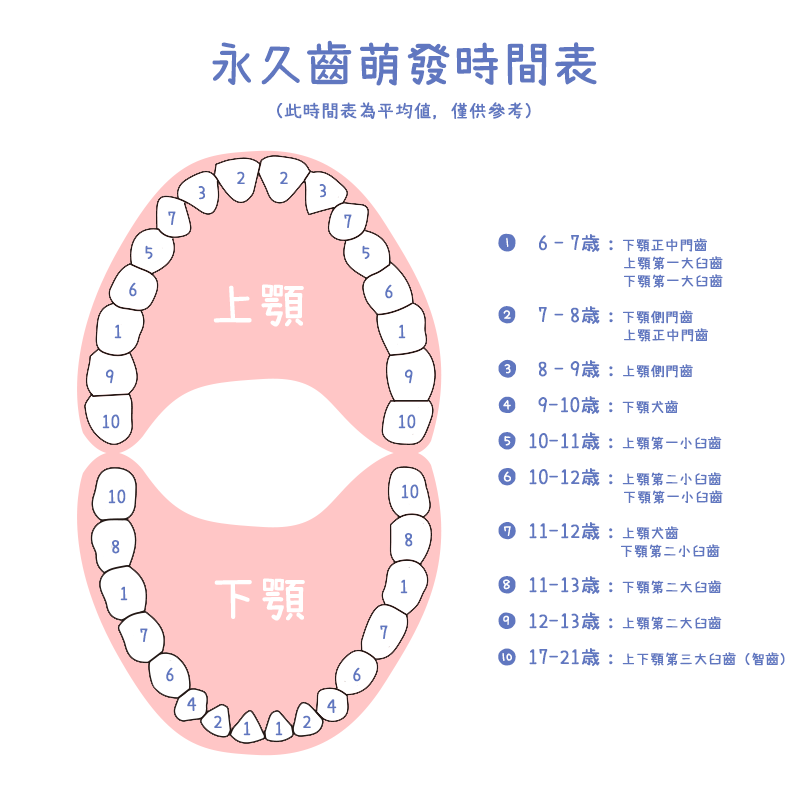
六至十二歲 Tooth growth and development, 6 to 12 years

六歲時,下顎前門齒與永久齒的第一大臼齒開始萌發。
這個時期家長最常問的問題就是:換牙時如果不先把乳牙拔除,新長的恆牙是否會長不好?
其實我們看到乳齒因為太晚拔除而影響恆齒發育的案例很少,所以家長不用為了要即時拔掉乳牙以免永久齒長歪而急著找牙醫師拔牙。
在下排門牙換牙時有時會看到新長的牙齒在乳齒的內側萌發出來,家長會很擔心這時候如果不拔牙新牙齒會長歪,其實永久齒的牙胚本來就在乳齒的舌側,萌發時沒有順利的將乳齒牙根完全吸收也是有可能的,所以新牙齒從乳牙內側長出來也不是甚麼罕見的狀況。
有時候,我們會看到小朋友的新舊牙齒並排出現在下顎門牙區。有些小朋友最怕拔牙,家長會想盡辦法威脅利誘小朋友接受乳牙拔除,其實這種情況並非一定要在這 個時候把乳牙拔除,過一段時間,新長的永久齒就會把乳齒往外推掉了。所以遇到這種情況,家長不用為了逼小朋友拔牙而讓親子關係緊繃。
小朋友擁有整齊潔白的乳牙是家長的驕傲,但是這一切的美好將在下門牙換牙時開始走山。
「為什麼新長的牙齒又黃又不整齊?」、「是不是以後一定要矯正呢?」這些都是家長常問的問題。
其實這崩壞的原因是新長的永久齒比舊的乳齒大,如果乳牙齒列沒有多餘的空間,新的永久齒就會沒有足夠空間排列整齊。
有些家長會問:那可不可以先把旁邊的犬齒拔除,騰出空間給新長的門牙使用呢?
雖然這可以解決門齒擁擠問題,但是這是向之後要萌發的犬齒借空間用,而且我們觀察到提前拔掉乳犬齒容易造成新萌發的永久門齒往內倒,而且無法根本解決前牙 擁擠問題,另外還擔心對顎骨生長的刺激降低。所以,在衡量利弊得失之下,我們不建議刻意提前拔除乳犬齒。有時因為乳犬齒提早喪失,我們會建議製作空間維持 器以避免下顎門齒往舌側傾倒。還有,提前喪失單側的乳犬齒大多會造成門齒的中線偏移,這些都是需要請兒童牙科醫師評估與治療的狀況。
贅生齒(supernumerary tooth)是除了永久齒列牙齒應有的數目外多長的牙齒
贅生齒好發在上顎門牙區,形狀大多屬於錐形,與永久齒的形態不同。贅生齒萌發方向有些是和正常牙齒萌發方向相同,有一些會是相反方向,往鼻腔的方向生長,之前曾有新聞報導說鼻腔長出牙齒就是這種情況。
贅生齒大多在牙科檢查時拍攝上顎前牙區根尖X光片或是牙科全口X光片時發現。大多是家長因為小朋友的門牙牙縫過大或是門牙延遲生長要求檢查換牙狀況,拍X 光片時發現。贅生齒的問題是有時會佔用永久齒萌發需要的空間,進而影響永久齒的排列。有一些可能會影響矯正治療時牙齒的移動,如果條件許可的情況下,應該 要考慮手術拔除。
先天性缺牙(Congenital Missing Tooth/Teeth)是永久齒的數目少於應有的數目
缺牙數從一顆到多顆都 有可能。最常發生區域是小臼齒區與下顎門牙區,多顆缺牙有一些是某些全身性疾病的牙齒表現,例如外胚層增生不良(Ectodermal Dysplasias)、鎖骨臚骨發育不良(Cleidocranial Dysplasia)等疾病或是某些基因缺陷有多顆永久齒缺失的問題。
先天性缺牙的治療重點是缺牙區的重建與全口咬合考量。要保留原來的乳齒嗎?原來乳齒與之後要長的永久齒的大小差異要如何解決?還是要用矯正方式將缺牙區的縫隙關閉?還是要植牙重建?過渡期空間要如何處理?這些問題需要家長與牙科醫師進一步討論治療計畫。
永久齒的異位萌發(Ectopic Eruption)常發生在第一大臼齒或是上顎犬齒
異位萌發的發現通常是因為小朋友永久齒的萌發延遲或是乳臼齒咬東西時疼痛,經X光片檢查時發現。第一大臼齒的異位性萌發輕微的會導致永久齒萌發延遲,嚴重的會造成第二乳臼齒牙根吸收,進而導致乳臼齒提前喪失、影響永久齒萌發空間,最終產生齒列擁擠的問題。
治療此類問題會依照病情嚴重程度而訂定不同的治療計畫。有可能會對第一大臼齒施予局部矯正治療,向遠心推開;亦有可能將第二乳臼齒拔除後再施與空間再生與 空間維持治療;或是將第二乳臼齒拔除後等待之後的全口矯正治療。犬齒的異位萌發有可能會造成犬齒阻生、犬齒與鄰近牙齒錯位、鄰近牙齒牙根吸收等問題。為了 減少這些傷害,有時會提前進行矯正治療,矯正治療可能需要合併埋伏齒露出手術,將異位萌發的牙齒牽引至適當位置。
乳齒嚴重齲齒、外傷或是永久齒異位萌發可能會導致乳齒提前喪失。乳齒提前喪失可能會造成相鄰牙齒傾斜或位移,進而導致永久齒萌發空間不足。遇到這問題時, 兒童牙科醫師可能會建議幫小朋友安裝空間維持器或是做空間再生治療。在換牙時期做好空間管理,可以降低以後全口矯正的需要。
乳齒的外傷或是牙根尖嚴重發炎,可能會導致在下方發育中的永久齒表面變白或變黃等不同程度的牙釉質受損。這叫做Turner's tooth。另一種牙釉質發育異常為牙釉質發育不全(Amelogenesis Imperfecta),牙釉質發育不全與牙釉質生成的基因異常有關連,患病的牙齒會有不同程度的牙釉質缺失或是發育不良等臨床發現,依據嚴重程度與缺損 型態有多種不同的分類。患病的牙齒因為在牙齒外層擔任保護工作的牙釉質有缺陷,所以較容易發生齲齒、敏感、磨耗等問題。這些問題導致患病牙齒可能需要使用 牙冠保護,嚴重者甚至有能需要拔除。
小學時期的小朋友已經很少看到吸奶嘴的不良習慣,但是偶爾還是看到這樣的病例,有的小朋友會轉變成吸手指。長期吸奶嘴或手指可能會導致前牙開咬,影響牙弓 發育(發展成尖形V-shape的牙弓)最終影響牙齒排列。另外一個會影響牙齒排列的是吞嚥時舌頭往前伸的習慣,這會導致口腔周圍肌肉不協調、前牙開咬、 顎骨發育異常與呼吸道的狹窄,進而增加後續齒顎矯正的困難度與矯正後維持的穩定性。兒童牙科醫師看到這樣問題會建議家長儘早幫小朋友改正不良習慣,習慣的 改變相當不容易,某些類型的矯正裝置搭配肌肉訓練課程可以協助小朋友與家長改正這些問題,但是能否成功還是取決於小朋友的配合度與毅力。
近年來空氣汙染嚴重,小朋友有鼻子過敏問題的比例也愈來愈高。鼻子過敏、呼吸道不通暢慢慢會讓小朋友養成口呼吸習慣。家長對於小朋友口呼吸的問題只是覺得 嘴巴開開的不美觀,殊不知小朋友是處於呼吸不順暢的痛苦中,長期呼吸不順也會影響到學習與睡眠。長期口呼吸會導致口腔周圍肌肉不協調,進而影響牙齒排列與 顎骨發育,也就是臉會變醜。要改正口呼吸,第一步是要先排除呼吸道通暢度的問題,鼻息肉、鼻中膈彎曲、腺樣體肥大、扁桃腺腫大、因過敏導致分泌物增加都有 可能導致呼吸道不通暢,這些問題要請耳鼻喉科醫師幫忙解決。牙科部分,我們可以使用功能性矯正裝置搭配呼吸訓練,小朋友在長期持續的訓練下大多可以慢慢改 掉口呼吸問題。
許多家長會詢問說,小朋友班級上同學有人已經開始矯正治療了,我的小孩需要這時候開始治療嗎?還是要等換完牙後才開始矯正?以排列牙齒的矯正治療,最佳時 機是在乳牙都換成永久齒後開始。為什麼有一些小朋友在還沒換完牙就開始矯正治療呢?在這時期開始的矯正治療我們稱作為第一階段治療(phase I treatment),主要的目的是矯正會影響齒列或顎骨發育的不良因素。例如單側或雙側錯咬的門牙、上顎太窄造成的後牙錯咬、角度旋轉的門齒、異位萌發 造成空間喪失還有為了改正口腔不良習慣等情況會在此時期做第一階段矯正治療。第一階段治療完成後,可能休息一段時間,等換完牙後再進行第二階段治療;也有 可能是接著進行第二階段的治療;也有人完成第一階段治療後不需要再做第二階段治療,這些會因每位小朋友的狀況不同而有不同的治療需求。有些家長會誤以為第 一階段治療完成就是矯正治療結束,其實並不一定。
The central incisor and first molar of the mandible start to erupt at age 6. One of the most commonly asked questions by parents is, will the permanent tooth come out straight if the primary tooth is not extracted first?
Clinically we have seen few cases where the development of permanent teeth were affected because primary teeth were extracted too late. So it's not necessary for parents to go to a pediatric dentist to extract a baby tooth for the permanent tooth to come out straight. For the lower central incisors, sometimes you can see the emerging tooth is on the lingual side of the baby tooth. Some parents worry if the baby tooth is not extracted, the permanent tooth will be tilted. In fact the germ of the permanent tooth is located on the lingual side of the baby tooth. It's possible that the root of the baby tooth is not fully absorbed as the permanent one emerges. This is not an uncommon scenario.
Sometimes we would see children's old and new teeth are present in parallel in the lower dentition. Parents would try all kinds of “carrots and sticks” measures to convince kids to accept an extraction treatment. However, this is not necessary. As time goes by, the newly erupted permanent tooth will naturally push the baby one out. There's no need to force children to accept extractions and create tension between parents and children.
Parents often take pride in their children's straight, white teeth. However, all this beauty tends to derail after the lower incisors start to foliate.
“Why are the new adult teeth coming in yellow and not straight?”, “Will my child need orthodontic treatment later on?” These are some of the common questions from parents.
The reason is that the new permanent teeth are larger than the old baby teeth. If there's no more space available, the new permanent teeth can't align properly.
Some parents ask, can you extract the lateral incisor to make space for the permanent central incisor?
Although this can solve the issue of incisal crowding by borrowing space from the emerging lateral incisor, however, the prematurely extracted lateral incisor is likely to cause dumping of central incisor and does not solve anterior crowding. It's also likely to decrease the growth stimulus to mandibular bone. Therefore, with all things considered, it's not recommended to deliberately extract baby lateral incisors early. Sometimes when primary lateral incisors are lost prematurely, we'd advise to fabricate a space maintainer to avoid the lower central incisors collapsing palatally. Also, unilateral early loss of a primary lateral incisor often leads to midline deviation. These conditions should be further assessed by pediatric dentists.
Supernumerary teeth are teeth that appear in addition to the regular number of teeth.
Supernumerary teeth are commonly found in the upper central incisor zone, mostly in a conical shape, different from the normal shape of permanent teeth. Some supernumerary teeth erupt in the same direction as the permanent teeth while others erupt in the opposite direction towards the nose. There was previously a news coverage describing a tooth found in the nose as it was the case with supernumerary teeth.
Supernumerary teeth are mostly found when taking an apical X-ray in the upper anterior zone or a panoramic film. In most cases it's when parents request for an examination due to a large gap between the front teeth or delayed eruptions of central incisors.
The problem with supernumerary teeth is sometimes they occupy the space required for the permanent teeth to erupt and affect the development of permanent teeth. Some may affect orthodontic tooth movement. If the situation permits, surgical removal should be considered.
Congenital missing teeth is teeth that are absent in the adult dentition.
It's possible to miss one or several teeth. The most common missing teeth are premolars and lower central incisors. Multiple congenital missing teeth are sometimes dental symptoms caused by other systemic diseases, such as ectodermal dysplasias, cleidocranial dysplasia or other genetic defects.
The focus of treatment for congenital missing teeth is restoration of the missing teeth and full-mouth occlusion. How to reconcile the difference in size between primary and permanent teeth? How to close the space of the missing teeth? by orthodontic treatment or implant therapy? How to deal with the space during the transitional period? These questions should be discussed by parents and pediatric dentists.
Ectopic eruption of permanent teeth is commonly found in the first molar or upper lateral incisor.
Ectopic eruption is often detected by X-rays when the eruption of permanent teeth is delayed or children complain of pain in the primary molar when chewing.
The ectopic eruption of first molar can cause delayed eruption of permanent tooth or more severely, the root resorption of primary second molar, leading to its early loss and subsequent crowding of the permanent dentition.
The treatment of ectopic eruption varies based on the level of severity of the condition. It's possible to start with partial orthodontic treatment by distalizing the first molar or extracting the primary second molar and applying a space maintainer. Alternatively we can extract the primary second molar and wait for full-mouth orthodontic treatment.
Ectopic eruption of molars can cause molar impaction, and root resorption of adjacent teeth. Sometimes partial orthodontic treatment may be required to minimize these damages. Orthodontic treatment may involve eruption of impacted teeth or bringing the ectopic erupted tooth into the right position. Severe cavities, trauma or ectopic eruption of permanent teeth may cause baby teeth to shed prematurally. This can cause the adjacent teeth to collapse or drift, leading to insufficient space for eruption of permanent teeth. When confronted with this issue, pediatric dentists may suggest a space maintainer or therapy to regenerate space. Good space management during the transitional period may reduce the need for full-mouth orthodontic treatment.
Trauma or apical lesions to a baby tooth may lead to the growing permanent tooth turning white or yellow and a varying level of damage to the enamel, also known as the Turner's tooth. Another type of enamel abnormality is amelogenesis imperfecta and it's associated with a developmental defect of enamel and a genetic abnormality of enamel development. Patients suffering from this condition may have a varying level of enamel defects and can be described in different categories based on the level of severity and types of defects. Because the protective layer of the tooth, enamel, is defected, patients are more likely to suffer from cavities, high sensitivity and tooth erosion. These problems suggest the need for crowns to protect the teeth. Some may be faced with extractions if the problem is severe.
It's uncommon to see school-aged children to use pacifiers. However, occasionally we do find these cases of prolonged use of pacifiers in which children may switch to thumb-sucking. Long-term use of pacifiers or thumb-sucking affects the dental arch development(into a V-shape arch) and ultimately changes the dental alignment. Another habit that impacts the tooth alignment is tongue thrust during swallowing. This causes disharmony of dental muscles, anterior open bite and abnormal mandibular bone development and constricted airway, all of which increase the complexity of future orthodontic treatment and jeopardize the results' long-term stability. When pediatric dentists notice these bad habits in the clinic, parents are often advised on behavioral changes as soon as possible. However, it's never easy to change habits. There are certain orthodontic devices, combined with muscle training, that can help correct these problems. The ultimate key lies in children's adherence and perseverance.
In recent years air pollution has increased the allergy rate found in children. Nose allergies and a congested nose will slowly lead to a mouth breathing habit.
Parents may regard mouth breathing as an esthetic issue because of the mouth opening. What they fail to recognize is that it can cause a chronic discomfort for children due to problems with breathing. It also affects school performance and sleep.
Chronic mouth breathing causes oral muscular disharmony and affects the growth and development of tooth alignment and facial bones.
How to stop mouth breathing?
First, remove factors that cause nose congestion, including nasal polyps, nasal septum deviation, adenoid vegetation, tonsil hypertrophy and increased mucus due to allergies. Please consult an EMT doctor first.
From a pediatric dentist's perspective, we recommend long-term training using functional orthodontic devices, together with myofunctional therapy to correct a mouth-breathing problem.
Some parents may ask when I should let my child begin orthodontic treatment as they see other kids have begun. Should they wait until the permanent teeth have already erupted? The best timing to begin orthodontic treatment for alignment is when the permanent teeth have fully erupted. Why, in some cases, will orthodontic treatment start before the transition is fully completed? During this time we call it phase I treatment. Its main purpose is to eliminate factors that will negatively affect the development of dentition or mandibular bones, such as unilateral or bilateral anterior crossbite, posterior crossbite due to a narrow maxilla, rotated central incisors, space loss due to ectopic eruption and/or bad oral habits. After the completion of phase I treatment, the treatment may be suspended until phase II when the permanent teeth have fully erupted. It's also possible to immediately continue with phase II or stop altogether as phase II may not be required after phase I. The treatment course varies based on every child's situation. Some parents may mistake the end of phase I for the end of the whole treatment. It's not necessarily the case.
